
For those who are new to our “Healthcare Done Differently” blog series, welcome. We are happy you’re here and hope you enjoy learning about ways to lower healthcare costs.
Within this blog series, we focus on unpacking the Health Rosetta principles around health plans being LOCAL. Each step, represented by a different letter, helps health plan sponsors build a firm foundation on regaining control and using common-sense strategies to better manage employee healthcare spend.
In our June blog we covered Step 1 or “L”, which stands for Learn how to be liberated from the status quo. Picking up from Step 2 or “O”, which stands for Optimize health plan infrastructure, covered in our October blog, we will now discuss Step 3 or “C” for Carve out Pharmacy Benefit Manager (PBM). Coupled with why you need to carve out the health plan’s PBM, we will share a go-to Rx cost-savings solution from the BCF Group Playbook.

Americans pay more than 2.5 times as much for the exact same prescription drugs when compared with other developed countries. Why Is that?
The structure of the United States pharmaceutical system is often referred to as “death by a thousand cuts.” The transaction complexity and lack of transparency make identifying and removing hidden revenue streams almost impossible.
To demonstrate just how big the problem is, $340 billion goes through this bureaucratic maze where each stakeholder retains a portion of the medication cost as their piece of the pie.
Direct-to-consumer advertising also fuels higher costs.
Envision this scenario:
- Patients see new medications on TV and ask for them by name from their doctors,
- Doctors are courted by drug reps to prescribe their drugs,
- Neither the patient nor the doctor knows the price of the drug,
- The health plan is left paying whatever medications are allowed,
- It’s the perfect storm!
Lastly, and by far the most problematic, is big pharma gaming the system. Schemes like the ones listed below cost consumers billions each year.
- Pay-for-delay agreements, where a brand drug manufacturer simply pays a generic company not to launch a version of a drug.
- Restricting access to samples for generic testing. Generic drugmakers need to be able to purchase large amounts of sample brand-name products to conduct bioequivalence testing.
- Evergreening, whereby a drug manufacturer will make small alterations to a drug to extend the patent and therefore restricting biosimilars (e.g., generics).
- Thicketing, which involves deluging the Patent and Trademark Office and the courts with so many patents and applications that the system essentially locks up.
The Federal Trade Commission conservatively estimates these schemes cost U.S. consumers and taxpayers $3.5 billion in higher drug costs each year.
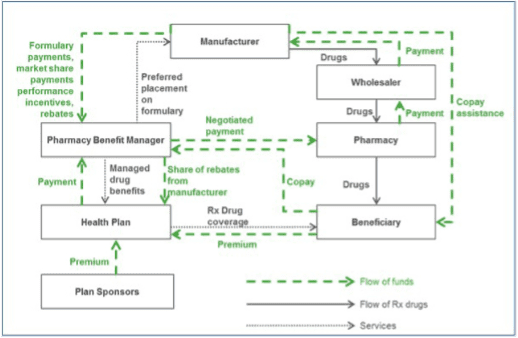
To further illustrate, The Wall Street Journal (WSJ) News Explainers video series “How Drug Prices Work” shows consumers how complicated and secretive drug pricing really is. In 2019, the WSJ explains how the flow of money, drugs, and rebates behind the scenes drives up the price of prescription drug medicine for consumers.
Given the state of the industry, you may ask yourself how employer-sponsored health plans pay less for medications.
Once again, we will reference the BCF Group Playbook, where our experience has shown that a fundamental first step for health plans is to work with an aligned Pharmacy Benefit Manager (PBM). Aligned PBMs will typically provide advantageous contract terms, including “pass-through” financial arrangements. This means that if an expensive brand name or specialty medication is filled using the health plan’s traditional channels, and not alternatively, the health plan will receive 100% of the manufacturer’s rebates for these medications. Predictably, PBM alignment is not typically found within prescription drug programs that are bundled into or owned by insurance carriers.
Another effective BCF Group Playbook cost-savings tool is alternative sourcing of medications. Health plans are now getting very creative in their efforts to gain the financial upper hand on Rx costs. Cost-savings strategies include:
- sourcing medications alternatively from other Tier 1 countries;
- excluding “new to market” medications from their formularies; and
- leveraging manufacturer’s assistance programs, where possible.
The concept is quite simple. To pay less for healthcare, you have to pay less for healthcare.
BCF Group clients have saved millions of dollars in drug costs using these and other similar strategies.
To learn more about charting a better path forward, we encourage you to continue reading our “Healthcare Done Differently” blog series. Next, we’ll dive into the “A” for “Add Value-based Primary Care” to your health plan. Learn how to provide concierge-style healthcare that delivers significantly higher member satisfaction ratings with $0 copay primary care. And again, within the next blog, we will touch on another go-to cost-savings solution from the BCF Group Playbook.